
Hydration in POTS Is Not Just About Drinking More Water
Understanding how salt, fluids, and blood volume work together is the key to improving symptoms and restoring physiological stability.
Most patients with POTS are told to drink more water. On the surface, that advice makes sense. If you feel lightheaded, fatigued, or unwell when standing, increasing fluid intake seems like a logical first step. The primary hydration goal for Postural Orthostatic Tachycardia Syndrome (POTS) is to expand blood volume to reduce orthostatic heart rate spikes from blood pooling. For POTS rehydration to work a combination of higher fluid intake, heavy sodium loading, and strategic planning is needed.
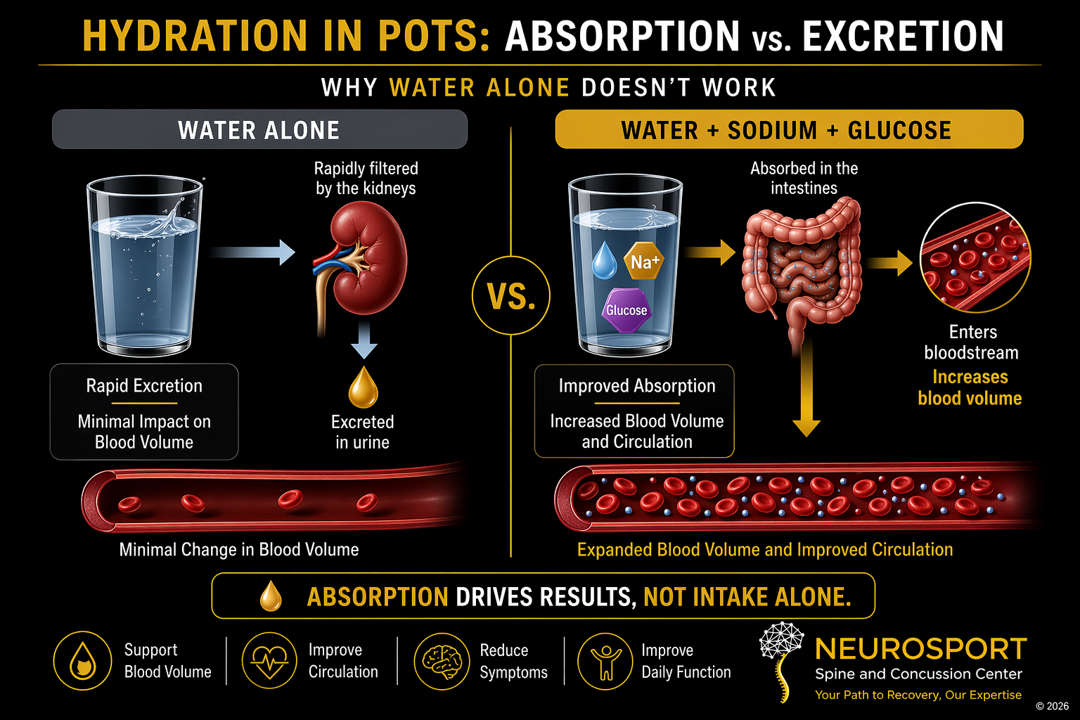
But for many patients, it doesn’t work. It is because the humans do not simply “hold onto” water, we carefully regulates fluid and electrolyte balance to maintain stability. When large amounts of plain water are consumed without the proper electrolyte support, the body responds by increasing urine production to maintain equilibrium. Much of what is consumed is lost rather than retained. This is why hydration strategies in POTS must go beyond water alone.
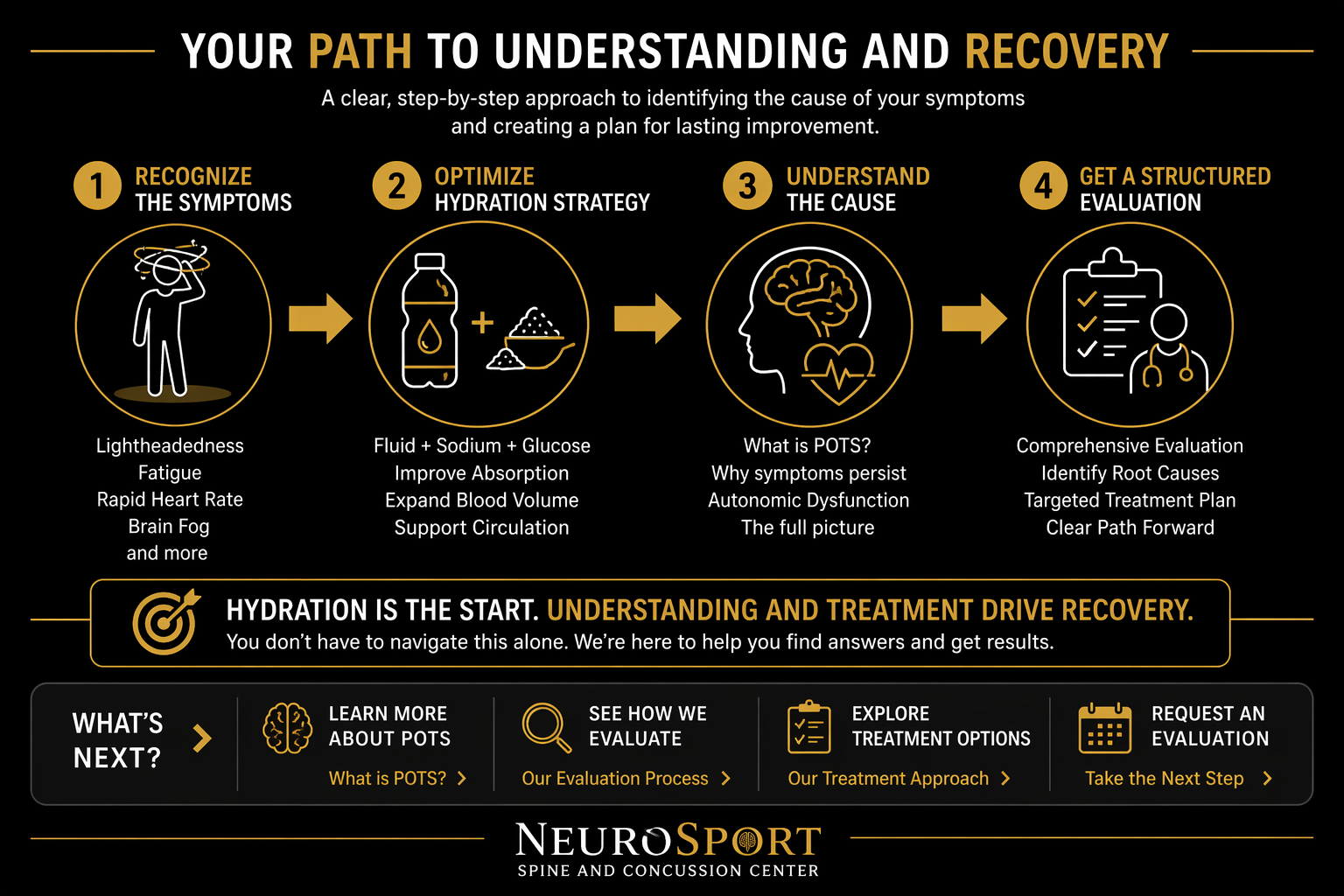
In POTS, the underlying issue often involves reduced effective blood volume and impaired autonomic regulation. When blood volume is insufficient, less blood returns to the heart when upright. The body compensates by increasing heart rate in an attempt to maintain blood flow to the brain. This leads to the hallmark symptoms patients experience:
Lightheadedness
Rapid heart rate
Fatigue
Brain fog
Exercise intolerance
Improving these symptoms requires more than increasing fluid intake. It requires a targeted strategy to support blood volume expansion and cardiovascular stability. When these elements are combined correctly, hydration becomes an effective clinical tool rather than a frustrating trial-and-error process. This page will walk you through what actually works and why.
Why Drinking More Water Alone Doesn’t Work
Most hydration advice for POTS starts and ends with one recommendation:
“Drink more water.”
While well-intentioned, this approach most often fails to improve symptoms and, in some cases, can make patients feel worse. To understand why, it is important to understand how the body regulates fluids. The human body maintains a tightly controlled balance of fluids and electrolytes. This balance is essential for maintaining blood pressure, circulation, and normal cellular function.
When large amounts of plain water are consumed:
Blood electrolyte concentration becomes diluted
The kidneys respond by increasing urine production
Excess water is rapidly excreted
The body is not trying to increase blood volume. It is trying to maintain blood electrolyte stability. As a result, simply drinking more water does not reliably increase circulating blood volume. This is a critical point for patients with POTS. If fluid intake does not lead to increased blood volume:
Circulatory support does not improve
The heart continues to compensate by increasing heart rate
Symptoms such as lightheadedness, fatigue, and brain fog persist
This is why many patients feel stuck despite following standard advice. Drinking more water without the appropriate electrolyte balance often leads to increased urination, not improved circulation. To make hydration effective, the goal must shift:
From drinking more fluids → retaining more fluids
Achieving this requires understanding how the body absorbs and holds onto fluid, which depends on the interaction between sodium, glucose, and water.
How the Body Actually Absorbs Fluids
Effective hydration depends on absorption, not just intake. Water does not move efficiently from the digestive tract into the bloodstream on its own. The body relies on specific transport mechanisms to move fluid into circulation and retain it.
One of the most important, but underrecognized, mechanisms of this function is the sodium-glucose cotransport system in the small intestine. When sodium and glucose are present together:
They are actively transported across the intestinal wall
Water follows this movement of sodium into the bloodstream
Circulating blood volume increases → there is less of a blood volume problem
This process is highly efficient and forms the basis of oral rehydration strategies used in medical settings. In practical terms, this means:
Water alone is poorly retained
Water with sodium is better
Water with sodium and glucose is most effective
This is the key reason why many hydration strategies fail in patients with POTS. Without the proper combination of sodium and glucose:
Fluid absorption is limited
Blood volume does not meaningfully increase
Symptoms persist despite increased intake
With the correct combination:
Fluid is absorbed more effectively
Blood volume expands
Circulatory stability improves
This is not about consuming large amounts of sugar. It is about using a small, targeted amount of glucose to enhance sodium absorption and improve fluid retention. For patients with POTS, this distinction is critical. Hydration must be structured to support absorption and retention, not just consumption.
The Goal: Expanding Blood Volume
In POTS, hydration is not simply about replacing fluids. The objective is to increase or expand effective circulating blood volume and improve cardiovascular stability when upright. When a healthy individual stands, typically the body rapidly adjusts:
Blood vessels constrict → Blood is returned efficiently to the heart → Blood pressure and circulation are maintained
In patients with POTS, this response is impaired.
When standing:
Blood pools in the legs and lower body → Less blood returns to the heart → Stroke volume decreases → The heart rate increases to compensate.
This compensatory increase in heart rate is what patients experience as tachycardia. Reduced blood flow to the brain contributes to:
Lightheadedness
Brain fog
Fatigue
Exercise intolerance
The goal of hydration and sodium intake is to improve this impaired physiology. By increasing blood volume:
More blood returns to the heart when upright
Stroke volume improves
The need for excessive heart rate compensation decreases
Symptoms become more manageable
This is why hydration strategies must be made with serious intent. Simply increasing fluid intake or eating more salt without improving absorption and retention does not meaningfully change this process. Effective strategies focus on:
Expanding circulating blood volume
Supporting vascular function
Reducing the physiological stress of standing
When blood volume improves, the entire system becomes more stable.
Common Hydration Mistakes in POTS and Dysautonomia
❌ Mistake #1: Drinking Large Amounts of Plain Water
Water without adequate sodium is often rapidly excreted. Many patients increase water intake but fail to improve blood volume because the fluid is not effectively retained.
❌ Mistake #2: Waiting Until Symptoms Appear
Hydration works best when it is proactive. Waiting until dizziness, fatigue, or tachycardia develops often means volume depletion has already occurred.
❌ Mistake #3: Ignoring Heat and Sweat Losses
Summer weather, exercise, hot showers, outdoor events, and travel can substantially increase fluid and sodium requirements. Many patients continue their usual hydration routine despite significantly increased losses.
❌ Mistake #4: Assuming All Electrolyte Products Are Equivalent
Some products are designed primarily for athletic hydration or flavor. Others are formulated around oral rehydration solution (ORS) principles that support sodium absorption and fluid retention. The label "electrolyte drink" does not guarantee clinical effectiveness.
❌ Mistake #5: Trying to Catch Up Later
Consuming large amounts of fluid at the end of the day is usually less effective than spreading fluids and electrolytes consistently throughout the day. Hydration is generally more effective when approached as a steady process rather than a rescue strategy.
The Takeaway
Most hydration failures are not caused by drinking too little water. They occur because the body is not effectively absorbing, retaining, or utilizing the fluids being consumed. For many patients with POTS and dysautonomia, success comes from combining adequate fluids, sufficient sodium, appropriate electrolyte selection, and consistent daily implementation.
Practical Hydration Targets
Once the goal shifts to improving absorption and increasing blood volume, hydration becomes a structured process rather than guesswork.
There is no single number that works for every patient, but there are clinically useful ranges that provide a starting point.
Daily Fluid Intake
Most patients benefit from a daily fluid intake in the range of:
2 to 3 electrolyte infused liters per day
This should be adjusted based on:
Body size
Activity level
Environmental conditions, especially heat
Symptom response
Fluid intake should be distributed throughout the day rather than consumed in large, infrequent amounts. Large boluses of plain water are less effective and may increase urine production without improving symptoms.
Daily Sodium Intake
Sodium intake is one key component of effective hydration in POTS. Typical clinical ranges fall between:
3,000 to 7,000 mg of sodium per day; this range should be individualized based on tolerance and response.
Sodium intake should:
Be spread across the day
Be paired with fluid intake
Be increased gradually if needed
Patients often underestimate how much sodium is required to influence blood volume. Small increases are often not sufficient to produce a meaningful physiological change.
Important Considerations
More is not always better. Excessive fluid intake without adequate electrolytes can worsen symptoms by increasing gastric upset, increasing urine production and diluting existing electrolyte balance. Similarly, abrupt increases in sodium intake without proper fluid support may lead to discomfort or poor tolerance. The goal is consistency and balance. Hydration strategies should be monitored and adjusted based on symptom response rather than applied as a fixed rule.
Clinical Caution
Patients with certain medical conditions should not significantly increase fluid or sodium intake without medical guidance. This includes individuals with:
Kidney disease
Heart disease or heart failure
Hypertension that is not well controlled
Those taking diuretics or medications that affect fluid balance
Endocrine or metabolic conditions affecting electrolyte regulation
In these cases, fluid and sodium strategies must be individualized and coordinated with the appropriate healthcare provider. If you are unsure whether these recommendations apply to you, a structured clinical evaluation is required before making significant changes.
Not All Electrolyte Supplements Work the Same
Many patients focus only on how much sodium a product contains. Sodium is important, but sodium alone is not the entire story.
One of the most important fluid absorption mechanisms in the human body is the sodium-glucose cotransporter (SGLT) located in the small intestine. This transport system moves sodium and glucose together across the intestinal wall. Water then follows this movement into the bloodstream. As sodium is absorbed water follows to increase the total volume of blood. The expansion increases plasma, the fluid component of blood, not the number of red blood cells.
As a result:
Consuming water alone is poorly absorbed if you are well hydrated and then excreted
Sodium improves fluid retention
Sodium plus a small amount of glucose improves absorption even further
Better absorption helps support plasma volume expansion and circulation
This is the same physiological principle used in oral rehydration solutions (ORS) worldwide. The goal is not simply consuming sodium. The goal is improving the body's ability to absorb and retain fluid.
Why “Zero Sugar” Is Not Always Better
Many patients with POTS intentionally choose zero-sugar electrolyte products because they believe avoiding sugar automatically creates a “cleaner” or healthier hydration strategy. In some situations, however, completely removing glucose may reduce hydration efficiency.
The small intestine absorbs sodium and water through specialized sodium-glucose cotransport mechanisms. These transporters use small amounts of glucose to help move sodium and fluid across the intestinal wall and into the bloodstream. This process is one of the physiologic foundations behind oral rehydration solutions (ORS).
This does not mean patients should consume large amounts of sugar or rely on traditional sports drinks. Many commercial sports beverages contain excessive sugar relative to sodium content and are designed primarily for athletic performance rather than plasma volume support.
Instead, the goal is balance.
For some patients with POTS and dysautonomia:
Plain water may be absorbed poorly
Very low sodium products may not adequately support blood volume
Completely sugar-free products may reduce sodium transport efficiency
Excessively sugary drinks may worsen gastrointestinal symptoms or blood sugar fluctuations
This is why some oral rehydration solutions outperform both plain water and many “wellness” electrolyte drinks.
The most effective hydration strategy depends on:
Symptom severity
Heat exposure
Activity level
Sweat losses
Gastrointestinal tolerance
Blood pooling severity
Underlying autonomic dysfunction
Some patients respond well to high-sodium products alone. Others benefit more from structured ORS-style hydration strategies designed to improve fluid absorption and plasma volume retention.
The clinical goal is not simply consuming more fluid. The goal is improving circulation, orthostatic tolerance, and autonomic stability.
Electrolyte Products: What Actually Helps
Not all electrolyte drinks are created with POTS physiology in mind.
Many commercially available products are designed for general hydration or athletic performance, not for increasing blood volume or improving autonomic function.
Understanding what to look for can make a meaningful difference.
What Matters in an Electrolyte Solution
An effective hydration strategy for POTS should include:
Adequate sodium content
A small amount of glucose to support absorption
A balance that promotes fluid retention rather than rapid excretion
Products that are low in sodium or lack glucose may not provide meaningful benefit, even if they are marketed as “electrolyte” drinks.
Electrolyte Product Comparison
Ranked by sodium content per serving. Sodium matters, but absorption matters too. Products that include a small amount of glucose may better support sodium and water absorption through sodium-glucose cotransport, which is why ORS-style products can be useful when the goal is blood volume support rather than simply flavoring water.
Electrolyte Products Ranked by Sodium Content
Higher sodium products may be more useful for patients with significant orthostatic intolerance, POTS, or orthostatic hypotension, but the best choice depends on clinical need, tolerance, fluid intake, and whether glucose-assisted absorption is desired.
| Product | Sodium | Glucose / Sugar | Best Use | Clinical Note |
|---|---|---|---|---|
| Trioral ORS | ~1,695 mg | Yes | High sodium need, OH, severe volume depletion | WHO-style ORS. Strong option when aggressive sodium and fluid replacement are needed. |
| LMNT | 1,000 mg | No | High sodium support | Good sodium load, but lacks glucose-assisted sodium absorption. Pair with food or carbohydrate if needed. |
| NormaLyte ORS | ~850-860 mg | Yes | POTS, dysautonomia, orthostatic intolerance | Strong ORS choice because glucose supports sodium absorption. |
| Pedialyte AdvancedCare Plus Powder | ~650 mg | Yes | Illness, dehydration, heat exposure | Good medical-style hydration product, more general dehydration focused. |
| Liquid I.V. Hydration Multiplier | ~500 mg | Yes | General hydration, travel, mild-moderate needs | Useful middle-ground product, but may be insufficient for higher sodium-demand patients. |
| Vitassium Capsules | 500 mg | No | POTS, OH, dysautonomia, sodium supplementation | Helpful when patients cannot tolerate sweet drinks or need portable sodium. Must be taken with fluid. |
| Thorne Daily Electrolytes | 480 mg | No sugar | Daily support, exercise, mild heat exposure | High-quality product and NSF Certified for Sport, but not ORS-style because it lacks glucose. |
| DripDrop ORS | ~330 mg | Yes | Daily hydration, mild-moderate symptoms, heat | Better absorption profile than plain water, but lower sodium than many POTS-focused options. |
| Nuun Sport | ~300 mg | Minimal / low sugar | Light activity, general hydration | Better for wellness or light activity than significant POTS/OH volume expansion. |
| Gatorade | ~250 mg | Yes, higher sugar | Athletic hydration | Familiar and accessible, but generally too low in sodium for many POTS patients. |
Key Takeaway
The highest sodium product is not always the best clinical choice. Effective hydration depends on sodium content, fluid volume, patient tolerance, and whether the product supports sodium absorption. A small amount of glucose can improve sodium and water absorption through sodium-glucose cotransport, which is why ORS-style products may outperform plain water or zero-sugar electrolyte drinks when the goal is blood volume support.
Remember: Many products labeled as “electrolyte drinks” are not formulated to improve blood volume in POTS, they might be best thought of as a sport drink. The goal is not just hydration. The goal is effective absorption and retention. Selecting or modifying electrolyte intake based on these principles can significantly improve outcomes.
Why Hydration Fails in POTS
Many patients with POTS feel frustrated because they are “drinking water all day” yet continue to experience dizziness, fatigue, tachycardia, heat intolerance, and exercise intolerance. The problem is that hydration involves far more than simply consuming fluids.
Water entering the stomach does not automatically translate into improved blood volume or better circulation. Effective hydration depends on fluid absorption, sodium transport, plasma volume retention, vascular control, and autonomic nervous system regulation.
Fluid Intake
Drinking water is the starting point, but fluid intake alone may not meaningfully improve circulation or orthostatic tolerance.Sodium Delivery
Sodium helps the body retain fluid within the bloodstream. Without adequate sodium, much of the water consumed may simply be excreted.Glucose-Assisted Absorption
Small amounts of glucose help transport sodium and water across the intestinal wall through sodium-glucose cotransport mechanisms. This is one reason some oral rehydration solutions work better than plain water or zero-sugar products alone.Plasma Volume Expansion
Once absorbed, retained fluid helps support circulating blood volume. Improved plasma volume may reduce dizziness, tachycardia, and symptoms related to blood pooling.Autonomic Regulation
Even with proper hydration, the autonomic nervous system still must regulate heart rate, blood pressure, vascular tone, and circulation. This is why hydration alone may not fully resolve symptoms in patients with significant autonomic dysfunction.
For many patients with POTS and dysautonomia, the clinical question is not simply, “Are you drinking enough water?” It is, “Is your body effectively absorbing, retaining, circulating, and regulating fluid?”
Hydration Alone May Not Be Enough
For some patients, improving hydration and sodium intake leads to meaningful symptom improvement. For others, symptoms persist despite aggressive fluid and electrolyte strategies. This occurs because POTS and dysautonomia are not simply “hydration problems.” They are disorders of autonomic regulation involving the body’s ability to coordinate circulation, vascular tone, heart rate, and blood pressure.
In many patients, hydration challenges are only one piece of a much larger physiologic problem.
Additional contributors may include:
Blood pooling in the legs or abdomen
Hypovolemia (low circulating blood volume)
Impaired vascular constriction
Neurocardiac axis dysfunction
Heat intolerance
Exercise intolerance
Gastrointestinal dysmotility
Post-concussion autonomic dysfunction
Connective tissue disorders such as hypermobile Ehlers-Danlos syndrome (hEDS)
Deconditioning following prolonged illness or injury
This is one reason patients with POTS often report:
“I drink water constantly but still feel dehydrated”
“Electrolytes help temporarily but symptoms return”
“I feel worse in heat”
“Standing still is harder than walking”
“My symptoms fluctuate dramatically day to day”
Hydration strategies may improve plasma volume and short-term symptom control, but they do not directly correct the underlying autonomic dysfunction driving many cases of POTS. At NeuroSport, we evaluate hydration status as part of a broader autonomic framework that may include:
Orthostatic testing
NASA Lean Test assessment
Heart rate and blood pressure analysis
Exercise intolerance evaluation
Blood pooling patterns
Oculomotor and neurological assessment
Post-concussion autonomic evaluation
Functional rehabilitation planning
The clinical goal is not simply helping patients drink more water. The goal is improving autonomic regulation, circulation, orthostatic tolerance, and overall function.
NeuroSport Balanced Electrolyte Formula (1 Liter)
A structured, high-sodium electrolyte solution designed to support fluid absorption, blood volume expansion, and electrolyte balance.
Ingredients
1 liter (4 cups) filtered or mineral water
1¼ teaspoons sea salt or Himalayan salt
(~2,300–2,500 mg sodium)¼ teaspoon potassium chloride (“salt substitute”)
(~350–450 mg potassium)Magnesium glycinate providing ~150–200 mg elemental magnesium
(powder or opened capsule)2 tablespoons lemon or lime juice
(improves taste and palatability)1–2 tablespoons honey or maple syrup
(~10–15 grams carbohydrate to support absorption)
Why This Formula Works
This formulation is designed to support multiple aspects of hydration and autonomic function:
Sodium supports plasma volume expansion and circulatory stability
Glucose enhances sodium absorption in the small intestine
Potassium supports cellular fluid balance and neuromuscular function
Magnesium supports neuromuscular stability and may reduce cramping or irritability
Fluid serves as the delivery system for absorption and circulation
This is not just hydration. It is a targeted strategy to improve absorption, retention, and distribution of fluid.
How to Use
Sip gradually over 30–60 minutes rather than consuming all at once
Use early in the day or prior to prolonged standing or activity
Can be used once or twice daily depending on individual needs
Adjust sweetness and concentration based on tolerance
Practical Considerations
Taste can be adjusted by modifying citrus or carbohydrate content
Start with lower volumes if you are not accustomed to higher sodium intake
Monitor symptoms and adjust intake accordingly
Clinical Note
This formulation provides a higher sodium load than many commercial products and may be more effective for patients with significant symptoms related to low circulating blood volume.
Practical Tips for Daily Implementation
Understanding hydration is one thing. Applying it consistently is what leads to improvement.
Most patients do not fail because of lack of effort. They struggle because the approach is not structured. These strategies help translate the physiology into daily habits that support symptom control.
Start Early in the Day
Hydration should begin in the morning, not after symptoms develop.
Begin fluid and electrolyte intake within the first 30–60 minutes of waking
Early intake helps establish blood volume before upright activity increases demand
Waiting until symptoms appear often means you are already behind. Thirst is a primitive sense. By the time you feel thirsty, your body is likely already 1% to 10% dehydrated, leading to reduced physical and cognitive performance.
Distribute Intake Throughout the Day
Large, infrequent fluid intake is less effective than steady intake.
Sipping fluids consistently rather than consuming large volumes at once
Pair fluid intake with sodium and electrolytes
Avoid relying on large boluses of plain water
Consistency supports better absorption and retention.
Use Electrolytes Strategically
Timing matters.
Use electrolyte solutions before prolonged standing, travel, or activity
Increase intake during heat exposure or illness
Consider a second serving later in the day if symptoms persist
Hydration should match physiological demand, not follow a fixed schedule.
Avoid Common Pitfalls
Several patterns commonly limit progress:
Drinking large amounts of plain water without electrolytes
Underestimating sodium needs
Inconsistent daily intake
Attempting to “catch up” after symptoms worsen
These approaches often lead to frustration without improving outcomes.
Adjust Based on Your Response
Every human is unique, there is no one-size-fits-all plan.
Monitor symptoms such as lightheadedness, fatigue, and heart rate response
Adjust fluid and sodium intake based on how your body responds
Increase gradually rather than making abrupt changes
The goal is to find a sustainable level that improves stability and function.
Heat and Environment Matter
Environmental factors significantly affect symptoms.
Increase fluid and electrolyte intake in hot weather
Know the summer hydration strategies for POTS
Be proactive before outdoor activity
Recognize that symptoms often worsen with heat and dehydration
Planning ahead can prevent symptom escalation.
Key Takeaway
Hydration in POTS is not a passive recommendation. It is an active, structured strategy that requires consistency, timing, and the right combination of fluids and electrolytes.
When applied correctly, these changes can lead to meaningful improvements in daily function and symptom control.
Download the NeuroSport: POTS Hydration Quick Guide
Patients do best when they have a simple, clear reference they can use daily. This guide summarizes the key points from this page into a practical, easy-to-follow format.
What the Guide Includes
Daily fluid targets
Sodium intake ranges
When and how to use electrolyte solutions
NeuroSport Balanced Electrolyte Formula
Key do’s and don’ts for effective hydration
Why This Matters
Hydration strategies are only effective when applied consistently.
A simple reference helps remove uncertainty and allows patients to implement these principles without overthinking the process.
Download the NeuroSport Hydration Guide 👉 POTS Hydration Quick Guide (PDF)
Use this as a daily reference to support consistency and improve symptom management.
Key Reminder
Hydration is not just about drinking more. It is about improving absorption, increasing blood volume, and supporting cardiovascular stability throughout the day.
Beyond Hydration: Addressing the Underlying Physiology
Hydration and electrolyte strategies are foundational in managing POTS. They can improve blood volume, reduce symptoms, and enhance daily function. However, they do not fully address the underlying problem. POTS is not only a fluid issue. It is a disorder of autonomic regulation, particularly involving the communication between the brain, heart, and blood vessels.
Even with optimal hydration:
Blood pooling may persist
Heart rate may remain elevated
Exercise intolerance may continue
This is because the system responsible for regulating these responses is not functioning efficiently.
The Next Step
To move beyond symptom management, treatment must target the underlying physiology.
This includes:
Improving autonomic control
Enhancing cardiovascular efficiency
Restoring tolerance to upright posture and activity
At NeuroSport, this is addressed through a structured, progressive approach known as the Moreau POTS Protocol (MPP).
Why This Matters
Hydration helps support the system.
Rehabilitation helps retrain the system.
Both are important.
Patients who combine effective hydration with targeted autonomic rehabilitation often experience more meaningful and sustained improvement.
Takeaway
If hydration strategies alone are not leading to improvement, it may be time to move beyond supportive care and address the underlying mechanisms driving symptoms.
A structured evaluation can help determine the most effective next step.
Not improving with hydration?
Hydration is only one part of POTS management.
Understanding the underlying cause is the next step.
👉 Learn what POTS actually is
👉 See how we evaluate these symptoms
👉 Request an evaluation
Request an Evaluation
Hydration helps support the system.
Rehabilitation helps retrain the system.
f you have been told to “drink more water” and are still experiencing symptoms, the issue is often not effort. It is the approach.
Persistent symptoms such as:
Lightheadedness
Rapid heart rate when standing
Fatigue or brain fog
Difficulty with daily activity
often indicate underlying dysfunction that requires a structured evaluation.
At NeuroSport, we assess patients with POTS and dysautonomia using a comprehensive, physiology-based approach designed to identify the cause of symptoms and guide targeted care. Hydration is an important starting point. For many patients, it is not the complete solution.
For many patients, hydration is not the entire answer. It is the starting point.
A structured evaluation can help determine what is missing and provide a clear path forward.