
Long COVID and Dysautonomia
Persistent symptoms after COVID infection are real, complex, and often misunderstood. While many individuals recover fully, others continue to experience lingering physiological dysfunction affecting the autonomic nervous system, exercise tolerance, circulation, and recovery capacity.
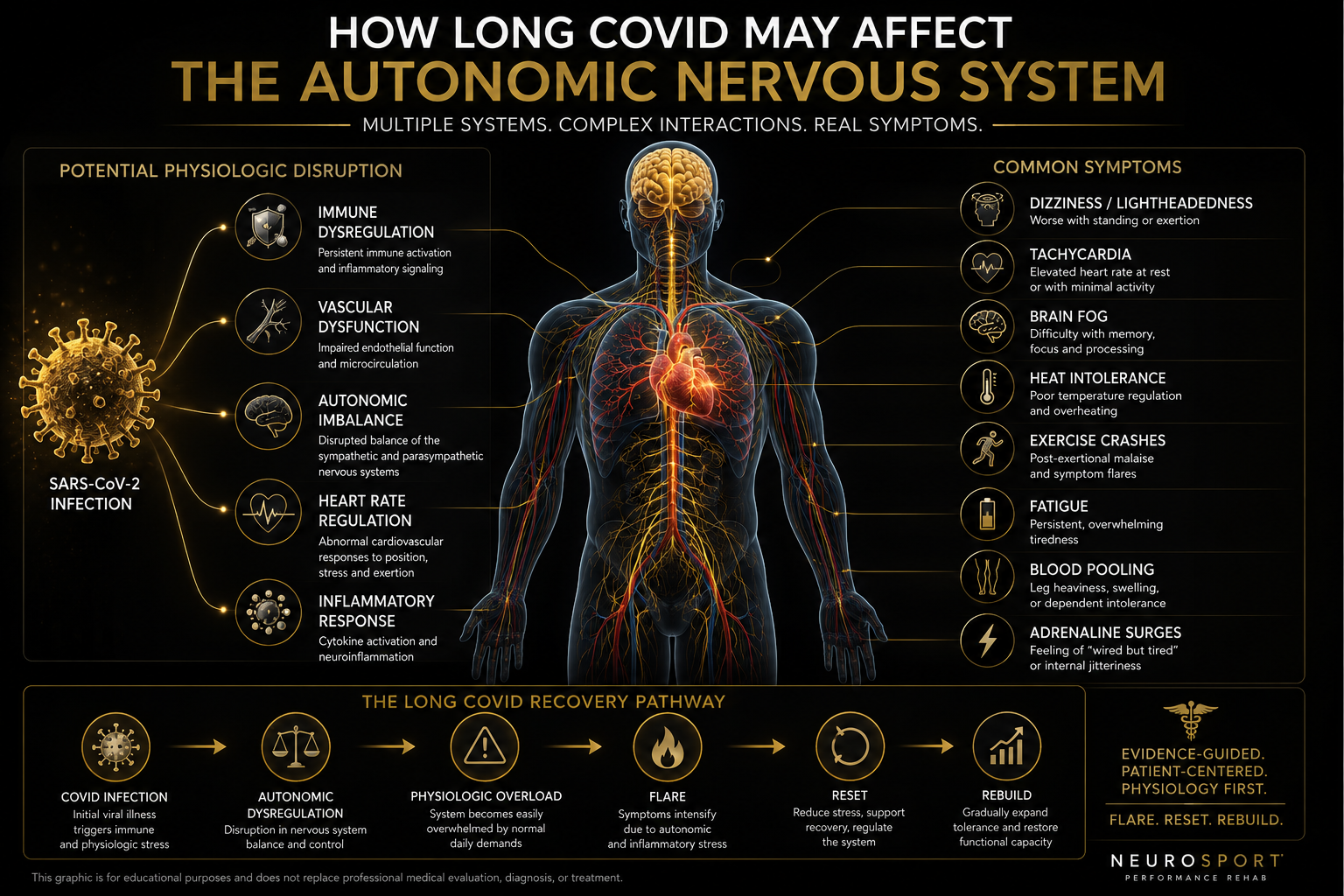
Patients may report dizziness, rapid heart rate, fatigue, brain fog, heat intolerance, post-exertional crashes, adrenaline surges, and difficulty returning to normal daily activity despite normal imaging or routine laboratory testing.
At NeuroSport, we evaluate these presentations through a systems-based lens focused on autonomic regulation, orthostatic physiology, exercise tolerance, and functional recovery.
This is not simply about “feeling tired.”
For many patients, it reflects disruption of the body’s ability to regulate blood flow, cardiovascular response, and physiologic stability under stress.
Recovery is often nonlinear.
The goal is not simply to push harder. The goal is to rebuild capacity intelligently, progressively, and safely.
Flare. Reset. Rebuild.
Long COVID Is More Than Fatigue
One of the most common frustrations reported by patients with Long COVID is being told that their symptoms are “just fatigue” or simply the result of deconditioning. While fatigue may be present, many individuals describe a much broader physiologic pattern involving the autonomic nervous system and the body’s ability to regulate circulation, exertion, and recovery.
Patients often report:
Rapid heart rate when standing
Dizziness or lightheadedness
Exercise intolerance
Brain fog or slowed cognition
Heat intolerance
Shortness of breath or “air hunger”
Palpitations
Tremulousness or internal shaking sensations
Poor recovery after physical or cognitive activity
Post-exertional symptom crashes
Difficulty tolerating busy environments or prolonged upright posture
For some individuals, even routine daily tasks such as grocery shopping, showering, climbing stairs, or attending social events can provoke significant symptom escalation.
In many cases, these symptoms reflect dysfunction involving the autonomic nervous system, the system responsible for regulating heart rate, blood pressure, vascular tone, temperature regulation, digestion, and physiologic adaptation to stress and activity.
This is one reason why many patients describe feeling “normal” one moment and profoundly limited the next. The issue is often not simply muscle strength or motivation. It is the body’s ability to regulate physiologic demand.
At NeuroSport, we frequently evaluate patients who were previously highly active, high functioning, and motivated before the onset of their symptoms. Many have already attempted to “push through” their condition, only to discover that excessive exertion can worsen autonomic instability and delay recovery.
Understanding the difference between simple fatigue and physiologic dysregulation is an important step toward building a more effective rehabilitation strategy.
What Is Dysautonomia?
Dysautonomia is a term used to describe dysfunction of the autonomic nervous system (ANS), the system responsible for regulating many of the body’s automatic functions.
The autonomic nervous system helps control:
Heart rate
Blood pressure
Blood vessel constriction
Breathing patterns
Temperature regulation
Digestion
Sweating
Exercise response
Recovery after physical or cognitive demand
Under normal conditions, the autonomic nervous system constantly makes rapid adjustments to help the body adapt to posture changes, activity, environmental stress, heat, dehydration, and exertion.
For example, when a person stands up, the nervous system should quickly tighten blood vessels and maintain adequate blood flow to the heart and brain. When this system becomes dysregulated, blood may pool in the legs or abdomen, heart rate may rise excessively, and symptoms such as dizziness, fatigue, palpitations, brain fog, and exercise intolerance can occur.
In some patients following COVID infection, the autonomic nervous system appears to become dysregulated or overly reactive, leading to persistent symptoms that may resemble POTS, orthostatic intolerance, or other autonomic dysfunction patterns.
This dysfunction may affect what we often describe clinically as the neurocardiac axis, the dynamic relationship between the brain, heart, blood vessels, and autonomic nervous system.
Importantly, dysautonomia is not always visible on standard imaging studies or routine laboratory testing. Many patients appear “normal” on conventional workups despite experiencing significant physiologic limitations during daily activity or upright posture.
At NeuroSport, we focus not only on symptoms, but also on how the body responds physiologically to standing, exertion, environmental stress, and recovery demands.
How COVID May Contribute to Dysautonomia
COVID infection has been associated with persistent autonomic symptoms in a subset of patients, including dizziness, rapid heart rate, palpitations, exercise intolerance, brain fog, heat intolerance, and post-exertional symptom crashes. These symptoms may resemble POTS, orthostatic intolerance, or broader dysautonomia patterns.
The exact mechanism is still being studied. Current evidence suggests that Long COVID is not explained by one single pathway. Instead, several overlapping mechanisms may contribute to autonomic dysfunction, including immune dysregulation, inflammation, endothelial dysfunction, small fiber nerve involvement, viral persistence or reactivation, mast cell activation, and autoimmunity.
The autonomic nervous system depends on rapid communication between the brain, heart, blood vessels, and peripheral nerves. If that signaling network becomes disrupted after infection, the body may have difficulty regulating blood pressure, vascular tone, heart rate, temperature control, and recovery after exertion.
This is why some patients feel reasonably stable at rest but develop significant symptoms when standing, walking, showering, exercising, eating, working, or trying to recover after activity. The system may not be failing structurally, but it may be poorly regulating physiologic demand.
At NeuroSport, we do not assume that every Long COVID symptom is dysautonomia. We evaluate for patterns of autonomic dysfunction using the clinical history, orthostatic testing, symptom provocation, heart rate and blood pressure responses, exercise tolerance, and recovery behavior.
The key clinical question is not simply, “Did COVID cause this?”
The better question is: Has COVID been followed by a measurable disruption in autonomic regulation, upright tolerance, and physiologic recovery capacity?
Common Symptoms Seen With Long COVID and Dysautonomia
Long COVID-related dysautonomia can present differently from one patient to another. Some patients primarily notice rapid heart rate and dizziness when standing. Others experience fatigue, brain fog, heat intolerance, adrenaline surges, or significant crashes after activity.
Common symptom patterns may include:
Rapid heart rate when standing or walking
Dizziness or lightheadedness
Palpitations or skipped-beat sensations
Chest pressure or air hunger
Fatigue that is disproportionate to activity level
Brain fog, slowed thinking, or word-finding difficulty
Heat intolerance
Sweating changes
Tremulousness or internal vibration sensations
Nausea or digestive changes
Blood pooling in the legs or hands
Head pressure or headache
Poor sleep quality
Adrenaline surges, especially at night or
after overexertionPost-exertional symptom crashes
These symptoms can be confusing because they may fluctuate significantly. A patient may tolerate one activity on one day and crash after the same activity on another day. That variability is part of what makes autonomic dysfunction so frustrating.
At NeuroSport, we look for patterns rather than isolated symptoms. The timing, triggers, posture dependence, exercise response, recovery time, and physiologic data often tell the story more clearly than the symptom list alone.
Why Recovery Often Feels Nonlinear
One of the most frustrating aspects of Long COVID and dysautonomia is that recovery rarely occurs in a straight line.
Many patients experience periods of improvement followed by unexpected setbacks or “flares.” A patient may begin tolerating more activity, feel encouraged, then suddenly experience a worsening of symptoms after physical exertion, cognitive overload, travel, illness, heat exposure, poor sleep, emotional stress, or even a series of smaller demands that collectively exceed physiologic capacity.
This does not necessarily mean the patient is “back to square one.”
In many cases, the autonomic nervous system is functioning with a narrower physiologic reserve. When the total demand placed on the system exceeds current tolerance, symptoms can escalate rapidly.
Patients often describe this as:
“crashing”
“hitting a wall”
“adrenaline dumping”
“shutting down”
“paying for it later”
For some individuals, the flare may last hours. For others, it may take days or even weeks to fully settle.
This is one reason why the traditional “push through it” approach can sometimes worsen recovery in patients with autonomic dysfunction or post-exertional symptom amplification.
At NeuroSport, we often explain this process using a capacity model:
The body has a limited amount of physiologic reserve available at a given point in recovery. When activity consistently exceeds that reserve, the autonomic system may become overloaded, leading to symptom escalation and delayed recovery.
This does not mean patients should avoid all activity. In fact, carefully structured rehabilitation is often important. The key is learning how to rebuild tolerance progressively without repeatedly triggering physiologic overload.
Flare → Reset → Rebuild
This framework is central to how many patients learn to navigate recovery:
Flare: Symptoms escalate after the system exceeds current physiologic tolerance.
Reset: The goal becomes calming the autonomic system, stabilizing physiology, and reducing overload.
Rebuild: Activity is gradually reintroduced in a controlled and progressive manner to improve long-term capacity.
Recovery is often less about forcing adaptation and more about intelligently expanding physiologic tolerance over time.
Long COVID and Exercise Intolerance
One of the hallmark features seen in many patients with Long COVID-related dysautonomia is exercise intolerance, a reduced ability to tolerate physical activity at levels that were previously manageable. For some individuals, even mild exertion may provoke:
Rapid heart rate
Dizziness
Shortness of breath
Tremulousness
Excessive fatigue
Head pressure
Brain fog
Symptom flares occurring hours later
Many patients describe feeling trapped between two frustrating realities:
Too little activity may contribute to deconditioning and reduced tolerance over time.
Too much activity may trigger physiologic overload and post-exertional symptom crashes.
This creates what is often called the “boom-bust cycle.” Patients may feel temporarily improved, attempt to resume normal activity too aggressively, then experience a significant setback that reduces tolerance again.
Importantly, exercise intolerance in Long COVID is not always explained by poor motivation, anxiety, or simple deconditioning alone. In many patients, the issue appears related to impaired autonomic regulation, abnormal cardiovascular responses to exertion, altered blood flow dynamics, or delayed physiologic recovery after activity.
This is why some patients can appear physically capable during short periods of activity but experience delayed symptom escalation afterward.
At NeuroSport, we emphasize that exercise itself is not inherently harmful. In many cases, appropriately structured rehabilitation is an important part of recovery. However, progression must be individualized and based on physiologic tolerance rather than forcing activity levels that repeatedly overwhelm the system.
The goal is not simply to exercise harder.
The goal is to improve the body’s ability to tolerate and recover from exertion more effectively over time.
This often requires:
Careful pacing strategies
Monitoring physiologic response to activity
Avoiding repeated overload cycles
Gradual progression of cardiac demand
Strategic recovery periods
Hydration and electrolyte optimization
Attention to sleep and autonomic recovery
For many patients, successful rehabilitation is less about intensity and more about consistency, progression, and physiologic adaptability.
Objective Evaluation Matters
One of the greatest frustrations for many patients with Long COVID and dysautonomia is hearing that “everything looks normal” despite ongoing symptoms and major functional limitations. In many cases, standard imaging studies and routine laboratory work may appear unremarkable. This does not necessarily mean the patient is functioning normally from a physiologic standpoint.
Autonomic dysfunction is often a functional regulation problem rather than a structural imaging problem. At NeuroSport, we focus on how the body responds to:
Upright posture
Orthostatic stress
Exercise demand
Recovery after exertion
Environmental stressors such as heat
Cognitive load and sensory stimulation
This is why objective physiologic testing can be important. Depending on the clinical presentation, evaluation may include:
Orthostatic heart rate and blood pressure analysis
NASA 10-Minute Lean Test
Exercise tolerance assessment
Heart rate variability trends
Symptom provocation patterns
Recovery response analysis
Oculomotor and vestibular screening when indicated
Functional activity tolerance evaluation
These assessments may help identify patterns consistent with orthostatic intolerance, autonomic instability, exercise intolerance, or impaired physiologic recovery.
Importantly, evaluation is not focused solely on obtaining a diagnosis label. The larger goal is understanding:
What triggers symptom escalation
How the autonomic system responds to stress and exertion
What physiologic patterns may be contributing to symptoms
How rehabilitation can be progressed more safely and effectively
For many patients, objective testing also provides validation that their symptoms are physiologic and measurable, not simply “in their head” or explained by lack of effort.
At NeuroSport, we believe that understanding the body’s physiologic response patterns is often the foundation for building a more individualized and sustainable recovery strategy.
NeuroSport Approach to Long COVID and Dysautonomia
At NeuroSport, we approach Long COVID-related dysautonomia through a systems-based rehabilitation model focused on autonomic regulation, physiologic tolerance, and functional recovery. No two patients present exactly the same way. Some individuals primarily struggle with orthostatic symptoms and rapid heart rate. Others experience exercise intolerance, post-exertional crashes, brain fog, heat intolerance, sleep disruption, or persistent autonomic overload.
Our goal is not simply to chase symptoms.
The goal is to understand how the body is responding physiologically and to build a more effective rehabilitation strategy around those findings.
Management may include:
Orthostatic and autonomic evaluation
Exercise tolerance assessment
Pacing and energy management strategies
Gradual progression of cardiac demand
Hydration and electrolyte support
Recovery optimization
Heat and environmental management strategies
Activity modification during flare periods
Objective symptom and physiologic tracking
Structured autonomic rehabilitation when appropriate
For selected patients with significant orthostatic intolerance or POTS-related features, rehabilitation strategies may incorporate principles from the Moreau POTS Protocol™, an exercise-based autonomic rehabilitation framework designed to progressively challenge and retrain autonomic regulation through carefully monitored physiologic demand.
An important part of recovery is recognizing that progression must often be individualized. Patients who repeatedly push beyond current physiologic tolerance may unintentionally prolong recovery through recurrent autonomic overload and post-exertional symptom escalation.
This does not mean patients should avoid activity altogether. In many cases, avoiding all activity may worsen long-term tolerance. Instead, the focus becomes:
Stabilizing the system
Improving recovery capacity
Gradually expanding physiologic tolerance
Reducing the frequency and severity of flares over time
At NeuroSport, we emphasize a rehabilitation approach that is progressive, measurable, and adaptable to the patient’s current physiologic capacity rather than forcing arbitrary timelines or one-size-fits-all exercise progression models.
When to Seek Evaluation
Persistent symptoms after COVID infection should not automatically be dismissed as simple fatigue, stress, anxiety, or deconditioning, especially when symptoms are interfering with normal daily function, upright tolerance, work, school, athletics, or recovery after activity.
Consider seeking evaluation if you are experiencing:
Dizziness or lightheadedness when standing
Rapid heart rate with upright posture or mild activity
Exercise intolerance or repeated post-exertional crashes
Brain fog or slowed cognitive processing
Heat intolerance
Palpitations or adrenaline surges
Difficulty tolerating busy environments or prolonged standing
Fatigue that feels disproportionate to activity level
Delayed recovery after physical or cognitive exertion
Symptoms that fluctuate unpredictably throughout the day
Persistent symptoms despite normal imaging or routine laboratory work
Evaluation may be especially important when symptoms persist for weeks or months after infection and are limiting the ability to return to normal function.
At NeuroSport, we focus on identifying physiologic response patterns that may contribute to persistent symptoms, including orthostatic intolerance, autonomic instability, impaired exercise tolerance, and recovery dysregulation.
The goal is not simply to assign a label.
The goal is to better understand how the system is functioning and to develop a more individualized strategy for rehabilitation and recovery.
Flare. Reset. Rebuild.
Recovery from Long COVID and dysautonomia is often nonlinear. Many patients improve not by forcing the system harder, but by learning how to stabilize physiology, rebuild tolerance progressively, and reduce repeated autonomic overload.
Frequently Asked Questions
Autonomic dysfunction often fluctuates based on sleep quality, hydration status, stress load, heat exposure, activity level, illness, hormonal factors, and cumulative physiologic demand. Many patients report that symptoms can vary significantly from one day to the next.
Can dysautonomia happen even if my MRI and blood work are normal?
Yes. Many autonomic disorders involve dysfunction in physiologic regulation rather than structural abnormalities visible on routine imaging studies. Patients may still experience significant functional limitations despite “normal” imaging or standard laboratory findings.
Is exercise good or bad for Long COVID and dysautonomia?
The answer is often nuanced. In many cases, appropriately structured rehabilitation and gradual activity progression can be helpful. However, repeatedly pushing beyond current physiologic tolerance may worsen symptom flares in some patients. Exercise progression often needs to be individualized and carefully monitored.
What is the difference between deconditioning and dysautonomia?
Deconditioning refers to reduced physical conditioning that can occur after inactivity. Dysautonomia involves dysfunction of the autonomic nervous system and physiologic regulation. The two can overlap, but they are not necessarily the same thing. Many patients with dysautonomia were previously highly active before symptom onset.
Can hydration and electrolytes help?
For some patients, hydration and electrolyte strategies may help support blood volume and orthostatic tolerance. However, electrolyte needs vary significantly between individuals and should be considered in the context of the patient’s symptoms, laboratory findings, blood pressure patterns, medications, kidney function, and overall clinical presentation.
How long does recovery take?
Recovery timelines vary widely. Some individuals improve gradually over several months, while others experience longer and more fluctuating recovery courses. Progress is often nonlinear, particularly in patients with autonomic dysfunction or post-exertional symptom amplification patterns. Our experience indicated that 8 - 16 months is fairly a fairly typical timeline.
When should I seek evaluation?
Evaluation may be appropriate when symptoms persist beyond the expected recovery period, interfere with normal function, worsen with standing or exertion, or significantly impact work, school, athletics, or daily activity tolerance.
Related Conditions and Topics
Long COVID-related dysautonomia often overlaps with other autonomic, neurologic, and exercise intolerance presentations. Patients may experience symptoms that resemble or coexist with several related conditions and physiologic patterns.
Explore related NeuroSport resources:
What Is POTS?
Understanding Postural Orthostatic Tachycardia Syndrome and orthostatic intolerance.Why Do I Feel Dizzy When I Stand Up?
Common causes of orthostatic symptoms and blood flow dysregulation.Dysautonomia Flares
Why symptom crashes occur and how physiologic overload may contribute to recovery setbacks.Electrolytes and POTS
Why sodium, hydration, glucose, and blood volume support matter.Hyperadrenergic POTS
Understanding adrenaline-driven autonomic presentations.Exercise Intolerance and Dysautonomia
Why exertion may trigger symptom escalation and delayed recovery.Brain Fog and Autonomic Dysfunction
The relationship between autonomic regulation, cognitive function, and mental fatigue.NASA 10-Minute Lean Test
Objective orthostatic testing and autonomic response evaluation.Moreau POTS Protocol™
NeuroSport’s rehabilitation-based approach to autonomic retraining and physiologic progression.
A Systems-Based Approach to Recovery
Long COVID and dysautonomia can affect far more than energy levels alone. These conditions may influence circulation, exercise tolerance, cognitive function, recovery capacity, sleep, heat tolerance, and the body’s ability to adapt to stress and activity demands.
At NeuroSport, we focus on understanding how the system is functioning physiologically, not simply whether imaging studies appear normal. Through objective evaluation, individualized rehabilitation strategies, and careful physiologic progression, the goal is to help patients improve tolerance, reduce autonomic overload, and progressively rebuild functional capacity.
Hydration helps support the system. Rehabilitation helps retrain the system.
Research and Clinical Understanding Continue to Evolve
Long COVID and dysautonomia remain active areas of ongoing medical research. While significant progress has been made in recognizing autonomic dysfunction following viral illness, many important questions regarding mechanisms, recovery timelines, and optimal rehabilitation strategies are still being investigated.
Current evidence suggests that Long COVID may involve multiple overlapping physiologic processes rather than a single isolated mechanism. This complexity helps explain why patients can present with very different symptom patterns and why recovery trajectories often vary significantly between individuals.
At NeuroSport, we believe it is important to approach these conditions with both scientific humility and clinical seriousness.
Patients experiencing persistent symptoms deserve:
Careful listening
Objective evaluation
Evidence-guided clinical reasoning
Thoughtful rehabilitation planning
Individualized progression strategies
At the same time, it is important to avoid oversimplified explanations, exaggerated claims, or one-size-fits-all treatment approaches.
Recovery may involve:
Improving autonomic regulation
Expanding physiologic tolerance
Reducing flare frequency
Optimizing recovery behaviors
Gradually rebuilding functional capacity over time
For many patients, progress occurs incrementally rather than all at once.
The encouraging reality is that many individuals do improve, especially when physiologic overload patterns are recognized early and rehabilitation strategies are aligned with the patient’s current tolerance and recovery capacity.
Request an Evaluation
Persistent symptoms after COVID infection can be frustrating, isolating, and difficult to explain, especially when standard testing appears normal but daily function remains significantly affected. At NeuroSport, we evaluate patients with complex autonomic and exercise intolerance presentations using a systems-based approach focused on physiologic function, orthostatic tolerance, recovery capacity, and autonomic regulation.
Patients commonly seek evaluation for:
Persistent dizziness or lightheadedness
Rapid heart rate with standing or activity
Exercise intolerance
Post-exertional symptom crashes
Brain fog and cognitive fatigue
Heat intolerance
Adrenaline surges or autonomic overload
Difficulty returning to work, school, athletics, or normal daily activity
Persistent symptoms despite prior evaluations or normal imaging studies
Our clinical approach emphasizes:
Objective physiologic assessment
Evidence-guided clinical reasoning
Individualized rehabilitation strategies
Progressive recovery planning
Functional restoration and tolerance building
Recovery is often not about forcing the system harder.
It is about understanding physiologic capacity, reducing repeated overload, and rebuilding tolerance progressively over time.
Struggling With Persistent Symptoms After COVID?
Persistent dizziness, rapid heart rate, exercise intolerance, brain fog, post-exertional crashes, and autonomic symptoms can significantly impact quality of life, even when routine imaging or laboratory studies appear normal.
At NeuroSport, we provide objective evaluation and individualized rehabilitation strategies focused on autonomic regulation, physiologic tolerance, and functional recovery.