
Exercise Intolerance in Concussion & Dysautonomia
Why Activity Can Trigger Symptoms, Fatigue, Dizziness, and Delayed Recovery
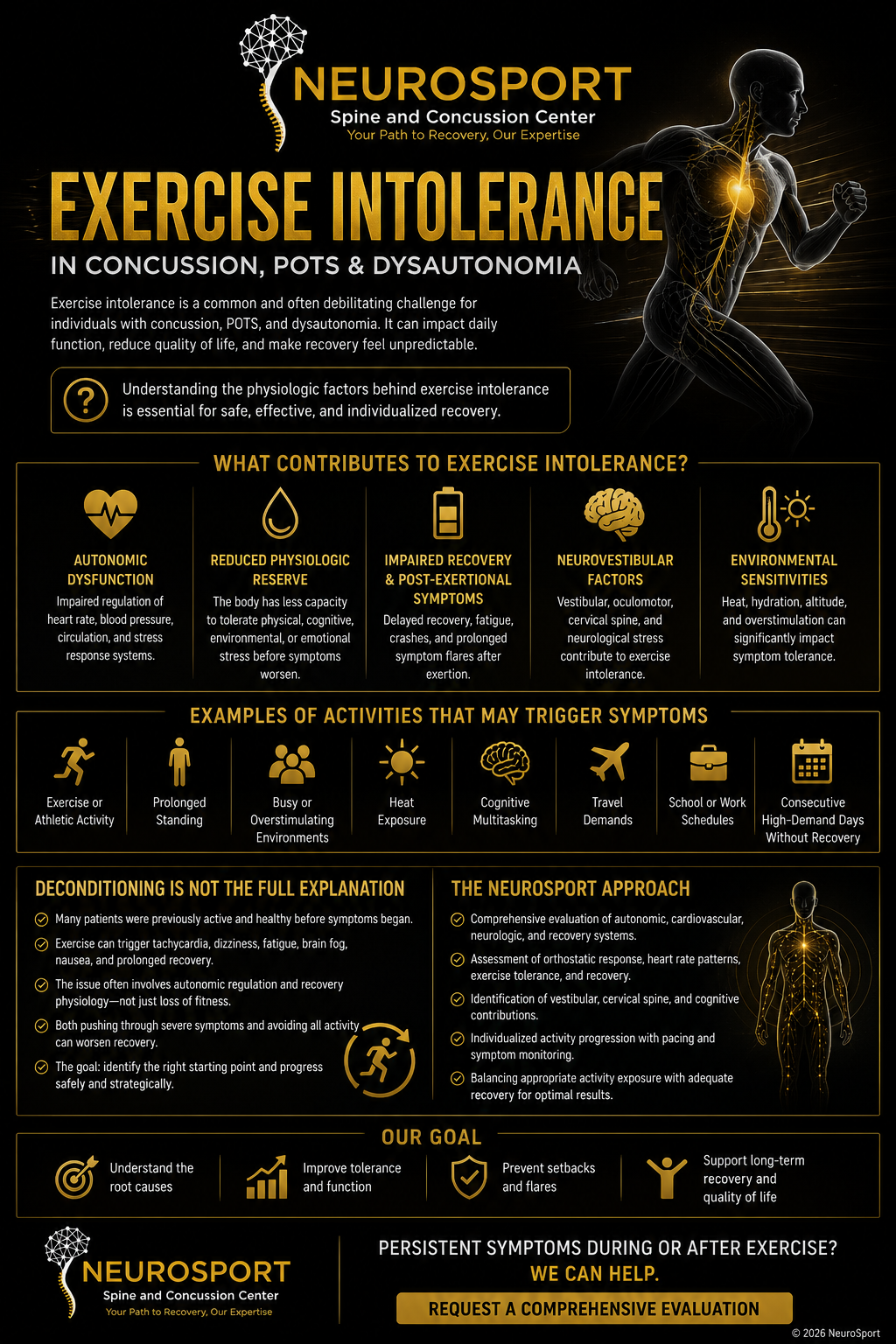
Exercise intolerance occurs when the body has difficulty tolerating physical activity at a level that should normally be manageable. This is a common problem for some people. In patients with concussion, POTS, and/or dysautonomia, symptoms may worsen with exercise because the autonomic nervous system, cardiovascular system, and recovery systems are not able to correctly regulating physiologic changes to meet exercise demands efficiently and correctly.
This dysfunction with exercise regulation can lead to dizziness, rapid heart rate, fatigue, brain fog, post-exertional symptom flares, nausea, fainting or near fainting and delayed recovery during and after activity.
Why Exercise Suddenly Feels Different
Many patients with concussion, POTS, or dysautonomia describe a dramatic unwanted change in how their body responds to physical activity. Activities that were previously easy or routine may suddenly trigger dizziness, rapid heart rate, fatigue, brain fog, shortness of breath, nausea, or prolonged recovery afterward. Exercise can become impossible to do because of these symptoms.
Some individuals with these conditions notice symptoms during exercise, while others feel relatively functional during activity but experience worsening symptoms during exercise, hours after exercise or even the next day. This delayed adverse physiologic response is often frustrating and confusing, particularly for active individuals who were previously able to tolerate high levels of physical or cognitive demand.
In people with dysautonomia, POTS and many cases, the issue is not simply “being out of shape.” Exercise intolerance in concussion and dysautonomia often reflects dysfunction involving autonomic regulation, cardiovascular response, blood flow control, physiologic recovery systems, and the body’s ability to adapt to exertional stress.
The autonomic nervous system plays a major role in exercise regulation. During activity, the body must continuously adjust heart rate, blood pressure, breathing patterns, blood vessel tone, temperature regulation, and energy utilization in real time. When these systems become dysregulated, even modest activity may create physiologic stress that exceeds the body’s current recovery capacity.
This helps explain why some patients feel disproportionately exhausted or symptomatic following activity levels that would normally be considered manageable.
The Autonomic Nervous System and Exercise Regulation
Exercise places significant physiologic demand on the body. During activity, the autonomic nervous system must continuously regulate heart rate, blood pressure, circulation, breathing patterns, temperature control, blood vessel tone, and recovery response in order to maintain stable performance. In healthy individuals, these systems adapt automatically and efficiently during exercise. Blood flow increases appropriately, cardiovascular demand is regulated smoothly, and recovery systems help restore physiologic balance after exertion.
In patients with concussion, POTS, or dysautonomia, this regulation process may become impaired.
Examples may include:
Excessive heart rate response during activity
Inadequate blood vessel constriction
Blood pooling in the extremities or abdomen
Reduced cerebral blood flow regulation
Impaired temperature regulation
Delayed autonomic recovery after exertion
Overactivation of sympathetic (“fight or flight”) pathways
Reduced physiologic reserve during physical or cognitive demand
When these systems become dysregulated, exercise may create physiologic stress that exceeds the body’s current adaptive capacity. As a result, patients may experience worsening symptoms either during activity or during the recovery period afterward.
This physiologic mismatch helps explain why some individuals feel significantly limited by activities that would normally be well tolerated, including walking, stairs, exercise, school activities, work demands, travel, or even prolonged upright posture.
In some patients, symptoms may improve gradually with carefully structured rehabilitation and progressive autonomic conditioning. However, inappropriate pacing, excessive exertion, or poorly tolerated exercise progression may worsen physiologic stress and contribute to symptom flares or delayed recovery.
Why Patients “Crash” After Activity
One of the most frustrating aspects of concussion and dysautonomia is that symptoms may worsen after activity rather than immediately during exertion itself. Many patients describe this as a “crash” or post-exertional flare. Common experiences may include:
Sudden exhaustion after activity
Worsening dizziness or lightheadedness
Increased brain fog or cognitive slowing
Head pressure or headache escalation
Increased heart rate instability
Nausea or sensory overload
Reduced upright tolerance
Feeling physically depleted for hours or days afterward
In some individuals, symptoms may not fully appear until several hours after physical or cognitive exertion. This delayed response can make it difficult for patients to recognize which activities are exceeding their current physiologic capacity. Several factors may contribute to post-exertional symptom worsening, including:
Impaired autonomic recovery regulation
Reduced physiologic reserve
Excessive sympathetic nervous system activation
Abnormal cardiovascular response to exertion
Inadequate blood flow regulation
Delayed recovery of neurologic systems after stress
Poor pacing or activity progression
Patients often become trapped in a cycle where they feel temporarily improved, attempt to resume normal activities too quickly, and then experience significant symptom worsening afterward.
This pattern is particularly common in concussion, POTS, dysautonomia, and post-viral autonomic dysfunction. In many cases, successful rehabilitation requires carefully balancing activity exposure with physiologic recovery capacity rather than simply “pushing through” symptoms.
Concussion and Exercise Intolerance
Exercise intolerance is common following concussion, particularly in patients with persistent symptoms or autonomic involvement. Many individuals notice that physical activity, busy environments, cognitive exertion, or rapid increases in activity level provoke symptoms that were not present prior to injury. Following concussion, multiple physiologic systems involved in exercise regulation may become disrupted, including:
Autonomic nervous system regulation
Cerebral blood flow control
Vestibular and balance systems
Oculomotor function
Sensory processing
Cardiovascular response
Recovery physiology
Cognitive endurance mechanisms
As a result, activities that previously felt routine may suddenly become physiologically demanding. Some patients experience:
Elevated heart rate during mild exertion
Dizziness with exercise
Head pressure or headache worsening
Visual or motion sensitivity during activity
Difficulty tolerating busy environments
Delayed fatigue after physical or cognitive exertion
Reduced exercise recovery capacity
Increased symptoms following school, work, sports, or travel demands
Importantly, concussion-related exercise intolerance is not always caused by structural injury visible on imaging. In many cases, symptoms reflect dysfunction in how the brain and autonomic nervous system regulate physiologic demand and recovery.
Historically, prolonged strict rest was commonly recommended after concussion. Current evidence now suggests that appropriately guided and symptom-monitored activity may be beneficial in many cases, particularly when exercise progression is individualized and carefully paced.
However, excessive exertion, aggressive return-to-play progression, or poorly tolerated activity advancement may worsen physiologic stress and contribute to prolonged symptom persistence in some patients.
At NeuroSport, evaluation focuses on understanding how concussion may be affecting autonomic regulation, exercise tolerance, recovery physiology, and activity capacity in order to better guide rehabilitation progression.
Dysautonomia and Reduced Physiologic Reserve
Many patients with dysautonomia or POTS experience a significant reduction in physiologic reserve, meaning the body has less capacity to tolerate physical, cognitive, environmental, or emotional stress before symptoms begin to worsen. Physiologic reserve refers to the body’s ability to adapt to changing demands while maintaining stable function. In healthy individuals, the autonomic nervous system continuously adjusts cardiovascular response, circulation, temperature regulation, breathing patterns, and recovery mechanisms in order to maintain balance during activity and stress.
In dysautonomia, these adaptive systems may become less efficient or unstable. As a result, activities that would normally require relatively modest physiologic effort may create disproportionate stress on the nervous system and cardiovascular system. Patients may feel as though their “energy battery” drains rapidly or that recovery following exertion takes far longer than expected.
Examples may include difficulty tolerating:
Exercise or athletic activity
Prolonged standing
Busy or overstimulating environments
Cognitive multitasking
School or work schedules
Consecutive high-demand days without adequate recovery
In some individuals, physiologic reserve fluctuates substantially from day to day. Patients may feel relatively functional one day and significantly limited the next depending upon sleep quality, hydration status, illness exposure, stress level, hormonal changes, environmental temperature, activity load, or cumulative physiologic demand.
This reduced adaptive capacity helps explain why many patients feel inconsistent, unpredictable, or easily overwhelmed by activities that were previously manageable before concussion, illness, or autonomic dysfunction developed.
Understanding reduced physiologic reserve is important when designing rehabilitation, pacing strategies, return-to-activity progression, exercise programs, school accommodations, or recovery planning in patients with concussion and dysautonomia.
Why Deconditioning Is Not the Full Explanation
Patients with concussion, POTS, or dysautonomia are sometimes told that their symptoms are caused entirely by “deconditioning.” While prolonged inactivity can certainly contribute to reduced fitness and exercise tolerance, deconditioning alone often does not fully explain the physiologic patterns seen in many autonomic and post-concussion presentations.
Many patients were previously healthy, athletic, active, or highly functional before the onset of symptoms. In some cases, exercise intolerance develops rapidly following concussion, viral illness, physiologic stress, or autonomic disruption rather than gradually over years of inactivity. Additionally, many individuals with dysautonomia continue attempting to remain active despite worsening symptoms. Patients frequently describe situations where exercise itself triggers dizziness, tachycardia, fatigue, nausea, brain fog, post-exertional crashes, or prolonged recovery periods.
In these cases, the issue may involve dysfunction in autonomic regulation, cardiovascular adaptation, blood flow control, or recovery physiology rather than simple loss of fitness alone. This distinction is important because inappropriate exercise progression or “pushing through” severe symptoms may worsen physiologic stress in some individuals. Conversely, excessive inactivity and prolonged avoidance of movement may also contribute to reduced conditioning and worsening tolerance over time.
The goal is not to avoid activity indefinitely, but rather to identify a safe appropriate physiologic starting point and progress rehabilitation in a structured and tolerable manner.
At NeuroSport, exercise intolerance is viewed through a physiologic and systems-based lens that considers autonomic regulation, recovery capacity, symptom response, cardiovascular adaptation, and activity tolerance rather than relying on deconditioning alone as the explanation for persistent symptoms. In fact we use carefully designed exercise as a treatment modality!
The NeuroSport Approach to Exercise Intolerance
At NeuroSport, evaluation of exercise intolerance focuses on understanding how physiologic systems are functioning together rather than simply determining whether a patient can or cannot exercise.
Many patients with concussion, dysautonomia, or autonomic dysfunction present with overlapping factors involving autonomic regulation, cardiovascular response, vestibular function, cervical spine dysfunction, recovery physiology, cognitive endurance, and symptom tolerance under exertional demand. Evaluation may include assessment of:
Orthostatic response patterns
Heart rate and physiologic response to activity
Exercise tolerance and recovery behavior
Symptom response during exertion
Oculomotor and vestibular contribution
Recovery pacing capacity
Cervical spine involvement
Activity tolerance patterns throughout the day
The goal is not simply to “push through” symptoms, but to better understand the physiologic mechanisms contributing to exercise intolerance and delayed recovery. In many cases, rehabilitation is most successful when activity progression is individualized, symptom-monitored, and carefully matched to the patient’s current physiologic capacity. Recovery often involves balancing appropriate activity exposure with adequate autonomic and physiologic recovery rather than relying on either excessive rest or excessive exertion alone.
At NeuroSport, emphasis is placed on structured evaluation, physiologic understanding, and individualized progression strategies designed to support recovery while minimizing unnecessary symptom escalation or post-exertional crashes.
Persistent Symptoms During or After Exercise?
Exercise intolerance in concussion and dysautonomia is often complex and highly individualized. Symptoms may involve autonomic dysfunction, altered cardiovascular response, impaired recovery regulation, vestibular involvement, reduced physiologic reserve, or overlapping neurologic stress responses that are not always visible on standard imaging studies.
NeuroSport specializes in structured evaluation for concussion, autonomic dysfunction, exercise intolerance, and persistent post-exertional symptom patterns.
Persistent Symptoms During or After Exercise?
Exercise intolerance in concussion and dysautonomia is often complex and highly individualized. Symptoms may involve autonomic dysfunction, altered cardiovascular response, impaired recovery regulation, vestibular involvement, reduced physiologic reserve, or overlapping neurologic stress responses that are not always visible on standard imaging studies.
NeuroSport specializes in structured evaluation for concussion, autonomic dysfunction, exercise intolerance, and persistent post-exertional symptom patterns.
Further Information
Explore additional educational resources related to concussion, dysautonomia, autonomic dysfunction, exercise intolerance, and physiologic recovery.
POTS & Dysautonomia
Learn how autonomic dysfunction may affect circulation, heart rate regulation, fatigue, dizziness, cognitive function, and recovery physiology.
Dysautonomia Flares
Understand why symptoms may suddenly worsen following stress, illness, heat exposure, overexertion, travel, or prolonged activity.
Heat Intolerance & POTS
Explore how heat exposure may worsen autonomic dysfunction, circulation problems, dizziness, fatigue, and exercise intolerance.
Long COVID & Dysautonomia
Learn about the overlap between post-viral illness, autonomic dysfunction, fatigue, exercise intolerance, and prolonged recovery patterns.
Why Imaging May Appear Normal
Understand why concussion and autonomic dysfunction symptoms may persist despite MRI or CT imaging appearing relatively normal.
Concussion & Autonomic Dysfunction
Explore the relationship between concussion, autonomic regulation, dizziness, fatigue, exercise intolerance, and persistent symptoms.
Do You Have Persistent Symptoms During or After Exercise?
Exercise intolerance in concussion and dysautonomia is often complex and highly individualized. Symptoms may involve autonomic dysfunction, altered cardiovascular response, impaired recovery regulation, vestibular involvement, reduced physiologic reserve, or overlapping neurologic stress responses that are not always visible on standard imaging studies.
NeuroSport specializes in structured evaluation for concussion, autonomic dysfunction, exercise intolerance, and persistent post-exertional symptom patterns.